Today, #physio4fight will talk about squats. Find us on Facebook and leave your like so we can continue to do what we love: talk about exercises, fitness and physiotherapy.
A squat is a strength exercise in which the athlete lowers their hips from a standing position and then stands back up. Squat requires articular and muscular mobility, strength, balance and muscle control. During the descent of a squat, the hip and knee joints flex while the ankle joint dorsiflexes; conversely the hip and knee joints extend and the ankle joint plantarflexes when standing up. This is the basic form using the bodyweight but further resistance like dumbbells and kettlebells can also be added.
Some squat benefits you can see below:
1-It strengthens your core.
2-It reduces the risk of injury.
3-It rushes calories.
4-It strengthens the muscles of your lower body.
5-It boosts athletic ability and strength.
6-It variety helps with motivation.
7-It is a functional exercise.
Types of Squat.
There are a few but the most popular are:
Basic Squat
Single Leg Squat
Pistol Squat
Jump Squat
Bulgarian Squat
Overhead Squat
Landmine Squat
Spanish Squat
Squats are an excellent form of exercise using your own bodyweight and some level of mobility, flexibility and strength is required to complete this exercise . Furthermore, you must consider your fitness level, a gradual training progression and any particular limitation from a previous injury.
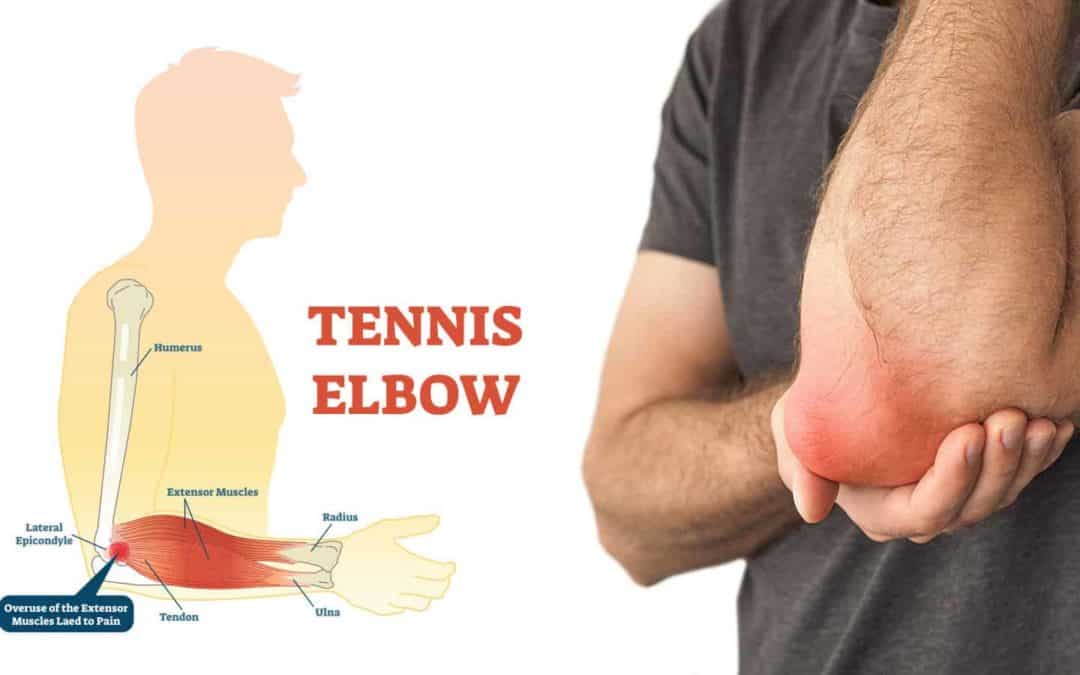
Lateral epicondylitis, also known as “Tennis Elbow”, is the most common overuse syndrome in the elbow. It is a tendinopathy injury involving the extensor muscles of the forearm. These muscles originate on the lateral epicondylar region of the distal humerus. In a lot of cases, the insertion of the extensor carpi radialis brevis is involved.
It should be remembered that only 5% of people suffering from tennis elbow relate the injury to tennis! Contractile overloads that chronically stress the tendon near the attachment on the humerus are the primary cause of epicondylitis. It occurs often in repetitive upper extremity activities such as computer use, heavy lifting, forceful forearm pronation and supination, and repetitive vibration. Despite the name you will also commonly see this chronic condition in other sports such as squash, badminton, baseball, swimming and field throwing events. People with repetitive one-sides movements in their jobs such as electricians, carpenters, gardeners , desk bound jobs also commonly present with this condition.
This is the most modern approach to deal with tendinopathy. Read more here.
There are several opinions concerning the cause of lateral epicondylitis:
1.Inflammation
Although the term epicondylitis implies the presence of an inflammatory condition, inflammation is present only in the earliest stages of the disease process.
2. Microscopic tearing
Nirschl and Pettrone attributed the cause to microscopic tearing with formation of reparative tissue (angiofibroblastic hyperplasia) in the origin of the extensor carpi radialis brevis (ECRB) muscle. This micro-tearing and repair response can lead to macroscopic tearing and structural failure of the origin of the ECRB muscle.
That microscopic or macroscopic tears of the common extensor origin were involved in the disease process, was postulated by Cyriax in 1936.
The first to describe macroscopic tearing in association with the histological findings were Coonrad and Hooper.
Histology of tissue samples shows “collagen disorientation, disorganisation, and fibre separation by increased proteoglycan content, increased cellularity, neovascularisation, with local necrosis.” Nirschl termed these histological findings bangiofibroblastic hyperplasia. The term has since been modified to bangiofibroblastic tendinosis. He noted that the tissue was characterised by disorganized, immature collagen formation with immature fibroblastic and vascular elements. This grey, friable tissue is found in association with varying degrees of tearing involving the extensor carpi radialis brevis.
3. Degenerative Process
The histopathological features of 11 patients who had lateral epicondylitis were examined by Regan et al. They determined that the cause of lateral epicondylitis was more indicative of a degenerative process than an inflammatory process. The condition is degenerative with increased fibroblasts, vascular hyperplasia, proteoglycans and glycosaminoglycans, and disorganized and immature collagen. Repetitive eccentric or concentric overloading of the extensor muscle mass is thought to be the cause of this angiofibroblastic tendinosis of the ECRB. Epicondylitis is a degenerative condition in which increased fibrolastic activity and granulation tissue formation occur within the tendon.
3. Hypovascularity
Because this tendinous region contains areas that are relatively hypovascular, the tendinous unit is unable to respond adequately to repetitive forces transmitted through the muscle, resulting in declining functional tolerance.
Clinical Presentation
The most prominent symptom of epicondylitis lateralis is pain, this pain can be produced by palpation on the extensor muscles origin on the lateral epicondyle. The pain can radiate upwards along the upper arm and downwards along the outside of the forearm and in rare cases even to the third and fourth fingers. Furthermore it is also often seen that the flexibility and strength in the wrist extensor and posterior shoulder muscles are deficient.
According to Warren, there are four stages on the development of this injury with regard to the intensity of the symptoms. 1. Faint pain a couple of hours after the provoking activity. 2. Pain at the end of or immediately after the provoking activity. 3. Pain during the provoking activity, which intensifies after ceasing that activity. 4. Constant pain, which prohibits any activity.
Furthermore it is also often seen that the flexibility and strength in the wrist extensor and posterior shoulder muscles are deficient. At least patients report weakness in their grip strength or difficulty carrying objects in their hand, especially with the elbow extended. This weakness is due to finger extensor and supinator weakness. Some people have a sense of paralysis but this is rare.
Symptoms last, on average, from 2 weeks to 2 years. 89% of the patients recover within 1 year without any treatment except perhaps avoidance of the painful movements .(sport injuries)
Assessment
A thorough assessment and examination are key elements in ensuring that the correct treatment plan is implemented, enhancing the recovery process. The assessment should also include elements to exclude a differential diagnosis.
Subjective Assessment
Onset of pain 24-72 hours after provocative activity involving wrist extension
Pain may radiate down forearm as far as the wrist and hand
Difficulty with lift and grip (Pain+/- weakness)
Changes in biomechanical factors- new tennis racquet, wet ball, over training, poor technique, shoulder injury
Objective Assessment
Pain and point tenderness over lateral epicondyle and/or 1-2 cm distal to epicondyle
Pain and weakness on resisted wrist extension
Weakness on grip strength testing (Dynamo-meter)
Pain and/or decreased movement on passive elbow extension, wrist flexion and ulnar deviation and pronation
Weak elbow extensors and flexors
Differential Diagnosis
Radial Tunnel Syndrome
Pain in the posterolateral area of the forearm
Pain sometimes spreads to the dorsal side of the wrist
Parasthesia
Weakness (overuse injuries of the musculoskeletal system)
The diagnose starts with asking about the activity level , occupation risk factors, recreational sports participation, medication and other medical problems. During the physical exam, the medicine will feel the structure of the elbow and other joints. Also the nerves, muscles, bones and skin are examined. It’s important to know which activities cause symptoms and where on your arm the symptoms occur.
Investigations
Investigations are usually not performed in the straightforward case of lateral elbow pain. However, in longstanding cases, plain X-ray (AP and lateral views) of the elbow may show osteochondritis dissecans, degenerative joint changes or evidence of heterotopic calcification.
Ultrasound examination may prove to be a useful diagnostic tool in the investigation of patients with lateral elbow pain. Ultrasound may demonstrate the degree of tendon damage as well as the presence of a bursa. X-rays: These may be taken to rule out arthritis of the elbow. 16% calcification along lateral epicondyle
Magnetic Resonance Imaging (MRI): if the symptoms are related to a neck problem, an MRI scan may be ordered. This will show if there is a possible herniated disk or arthritis in your neck. Both of these conditions often produce arm pain. MRI- 100% thickening[
Electromyography (EMG): An EMG is used to rule out nerve compression. Many nerves travel around the elbow, and the symptoms of nerve compression are similar to those of tennis elbow.
Treatment
a-We must understand that managing aggravating factors is vital.
b-We also must understand that tendons respond well to gradual loading.
c-It is a slow process
Your doctor may refer you to a physiotherapist if your tennis elbow is causing more severe or persistent pain. Physiotherapists are healthcare professionals who use a variety of methods to restore movement to injured areas of the body. The physiotherapist also will check for red flags, referred neck pain and will advice you how to find the best way to manage pain and flare-ups.
If you have tennis elbow, you should stop doing activities temporarily that strain affected muscles and tendons. During the acute phase, holding a cold compress, such as a bag of frozen peas wrapped in a towel, against your elbow for a few minutes several times a day can help ease the pain.
If you use your arms at work to carry out manual tasks, such as lifting, you may need to avoid these activities until the pain in your arm improves.
Alternatively, you may be able to modify the way you perform these types of movements so they do not place strain on your arm.
Your physiotherapist may use passive manual therapy techniques, such as massage and manipulation, to relieve pain and stiffness, and encourage blood flow to your arm. They can also show you active exercises you can do to keep your arm mobile and strengthen your forearm muscles. Research shows that tendons need some loading to get better and active treatment is very effective but it can take time. Try moving normally the best way you can without increasing the symptoms.
The use of an orthoses – such as a brace, strapping, support bandage or splint – may also be recommended in the short term.
Steroids are a type of medication that contain manmade versions of the hormone cortisol, and are sometimes used to treat particularly painful musculoskeletal problems.
Some people with tennis elbow may be offered steroid injections when other treatments haven’t worked.
Shockwave therapy is a non-invasive treatment, where high-energy shockwaves are passed through the skin to help relieve pain and promote movement in the affected area.
How many sessions you will need depends on the severity of your pain. You may have a local anaesthetic to reduce any pain or discomfort during the procedure.
The National Institute for Health and Care Excellence (NICE) states that shockwave therapy is safe, although it can cause minor side effects, including bruising and reddening of skin in the area being treated.
Research shows that shockwave therapy can help improve the pain of tennis elbow in some cases. However, it may not work in all cases, and further research is needed.
Surgery is rare and may be recommended as a last resort treatment in cases where tennis elbow is causing severe and persistent pain.
First of all thank you for support our Facebook page. You can like on Facebook Physio4fight here.
Today we will write about boxing, the noble art.
Boxing is a combat sport in which two people, usually wearing protective gloves, throw punches at each other for a predetermined amount of time in a boxing ring.
Amateur boxing is both an Olympic and Commonwealth Games sport and is a standard fixture in most international games—it also has its own World Championships. Boxing is probably one of the oldest sports ever.
Marco Ruas, the first hybrid MMA fighter and UFC champion
After Marco Ruas, the first hybrid MMA fighter and winner of the UFC 7, Boxing has started being used in mixed martial arts as well for multiple athletes. In a modern MMA era Boxing skills are mandatory.
Quick, explosive movement in boxing s demand both strength and motor skills. The athlete needs to be in control of the shoulders, back, hips, knees and ankles, all at the same time. Boxers need to be able to move in any direction quickly, smoothly and efficiently in order to avoid strikes and prepare for attacks.
The most common acute injuries among boxers are concussions, cuts and blows to the face, and injuries to the hands, fingers and wrists. There can also be muscular injuries from direct blows or from pulling muscles. Ankle sprains and dislocated shoulders are not uncommon. Many boxers are also susceptible to overuse injuries, which can cause long-lasting problems in the knees, calves and feet.
Wrist sprain. Due to poor wrist stability and trauma.
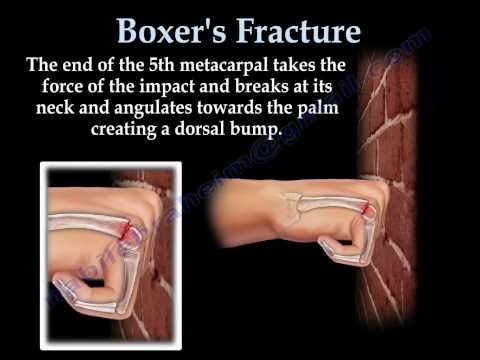
Hand fractures. A common injury is the boxer’s fracture (the break of the 5th metacarpal bones of the hand near the knuckle). Occasionally it is used to refer to fractures of the 4th metacarpal as well. Symptoms include pain and a depressed knuckle. Classically, it occurs after a person hits an hard object with a closed fist.
Finger sprain
Boxer’s knuckle. A boxer’s knuckle is a severe injury of the joint capsule frequently accompanied by an injury of the extensor apparatus. This injury can lead to a career-threatening situation for the athlete if not diagnosed and treated in a correct manner.
Bennett’s fracture. Bennett’s fracture is a break of the lower part of the first metacarpal bone. The fracture is often displaced. This means that the first metacarpal no longer sits correctly in the joint.
Dislocated shoulder. A dislocated shoulder is an injury in which your upper arm bone pops out of the cup-shaped socket that’s part of your shoulder blade. The shoulder is the body’s most mobile joint, which makes it susceptible to dislocation. This injury is common in many sports and some athletes are more prone to this injury due to poor shoulder stability.
Back pain
Neck pain
Achilles and shoulder tendinopathy. Tendinopathy, also known as tendinitis or tendonitis, is a type of tendon disorder that results in pain, swelling, and impaired function. The pain is typically worse with repetitive movements after increasing training volume suddenly.
Strain injuries in the shoulders, neck, back, knees, calves and feet
The guidance – the world’s first on returning to running after childbirth – was produced by pelvic health physios Emma Brockwell and Gráinne Donnelly and musculoskeletal physio Tom Goom.
‘The response was enormous and unexpected. It went international. Infographics were produced summarising the guidance document and these have since been translated into six languages by professional bodies in other countries, with more currently underway,’ Ms Brockwell said.
As a result, the trio were offered the opportunity to work alongside Dr Alan Rankin (sports medicine physician), Dr Hayley Mills (chartered psychologist) and Dr Marlize De Vivo (registered biokineticist and graduate sports rehabilitator) to produce an infographic based on the original guidance that aligns with the CMO physical activity guidelines.
The infographic was published in the British Journal of Sports Medicine in May and it is hoped to be the first in the series of publications on returning to running and high-impact exercise after having a baby.
‘The huge interest shows that there is a great need for this information. As well as being aligned with the CMO guidelines, we’ve been approached by academic institutions, which is great because it will help influence further research into this area.
‘Emma and I are also delighted to be appointed as associate perinatal physical activity research group team members at Canterbury Christ Church University’.
Today we are posting some videos from YouTube where multiple therapists and coaches are discussing running techniques. This subject is complex and should be assessed properly based on each individual.
The blog Physio4fight is purely a source of information and CANNOT replace the assessment of a qualified professional. We recommend seeking professional advice before embarking on any form of self treatment or training. The purpose of this post is ONLY for information.
Neither the content or nor any other service provided through Physio4fight is intended to be relied on for medical diagnosis or treatment. Never delay in seeking professional advice because of something seen on this blog.
What do you think about this subject? Leave your comment below.
Physiotherapists are calling on people to visit trusted sources online after a study highlighted alarming levels of misinformation in the most-watched back pain videos on YouTube.
Millions of searches are conducted each year for advice on common bone, muscle or joint problems, such as back, neck or shoulder pain, and will have been the first course of action for many people during the lockdown.
The Chartered Society of Physiotherapy enlisted a team of specialist musculoskeletal physiotherapists to study the 100 most highly viewed videos on YouTube when searching for ‘advice and treatment for back pain’.
Some of the videos had millions of views but the physiotherapists found:
-Almost half contained a myth (43%) -Six in 10 contained false or misleading information (60%) -Nearly a third had an unrealistic video demo (32%) -Four in 10 contained unhelpful language that was fear evoking or contradictory (42%) -Almost half did not state their qualifications for providing advice (45%) -Among the most egregious examples were videos that recommended applying garlic oil to the back, taking devil’s claw and avoiding ‘abnormal eating’.
Some claimed to have a ‘miracle cure’ for back pain – such as drinking lemon and salt – while others promised a ‘quick fix’.
Many pushed advice that would lead the viewer to believe their back was weak or easily damaged and movements such as bending or twisting should be avoided.
Physiotherapists say the study reflect a wider problem with unregulated health advice online, and reported regularly seeing the consequences in their clinics before the lockdown.
A snap poll of 100 physiotherapists found that nearly a third (32%) of their patients cited false or misleading information they got from the internet on a daily basis.
Two thirds (66%) of physiotherapists said they had to treat patients whose condition had worsened because of this.
The CSP has worked with NHS England, Public Health England, Versus Arthritis, The British Orthopaedic Association (BOA), The British Society for Rheumatology (BSR), and the Arthritis and Musculoskeletal Alliance (ARMA) to create a hub of evidence-based online advice for common problems such as back or neck pain.
Physiotherapists are reporting treating an emerging number of patients with ‘isolation injuries’ due to doing unfamiliar exercise programmes, suddenly doing lots of garden and doing odd jobs around the house.
Chartered Physiotherapist, Lisa Osborn-Jenkins, who led on the research, said:
‘We weren’t surprised at the amount of misinformation we found online as it’s reflected at our clinics when patients arrive fearful with unhelpful beliefs and expectations of treatments that may help.
‘We are particularly concerned that during this difficult period for all of us, many people are doing everything they can to avoid placing added pressure on healthcare workers so may be relying more on advice they find online. Our lives have become more digital through the current challenges and yet there is a mind-field of online advice available.
‘The public need to be aware that this information isn’t regulated and with a click of your mouse you risk receiving biased, unhelpful and incomplete advice.’
Andy Bennett, NHS England’s national clinical director for musculoskeletal conditions, said:
‘It’s understandable that people in pain could be drawn to advice that offers quick fixes, but these ‘treatments’ can often make matters worse, which is why it’s critical that people can access the right advice to help manage their pain. I would urge anyone with bone, joint or muscle pain to visit reliable sources of information whether this is the NHS website or the CSP hub and seek treatment if they need it through a GP or 111.’
People are getting more active now (this is actually good) and sometimes we can get injured during or after exercising. Physiotherapy is normally advised and is an effective treatment.
However, there are scenarios that can be more complex and physiotherapy is not the answer. We are talking about red flags in physiotherapy.
Red flags are prognostic signs and symptoms suggestive of serious pathology. They are RARE (many physios work the whole life and do not see any or just a few cases) but can be concealed as a “joint/ muscle pain” but in fact they are something else and more sinister.
See some red flags below:
-Neck pain is quite common BUT if your symptoms are…
pain is getting much worse ( It can be individual and subjective due to multiple factors)
lack of co-ordination – for example trouble with tasks like buttoning a shirt
heaviness or weakness in your arms or legs
pins and needles (normally both arms but can affect just one arm) in an arm as well as pain
problems when walking
loss of bladder or bowel control
These can be signs of a more severe condition (cervical myelopathy) which can cause permanent damage to the spine if left untreated.
-Lower back pain is quite common BUT if you are having…
sciatica on both sides
weakness or numbness in both legs that is severe or getting worse
numbness around or under your genitals, or around your anus
finding it hard to start peeing, can’t pee or can’t control when you pee – and this isn’t normal for you
you don’t notice when you need to poo or can’t control when you poo – and this isn’t normal for you
Gait can also be affected
Theses symptoms are related to cauda equina. Cauda equina syndrome is a rare and severe type of spinal stenosis where all of the nerves in the lower back suddenly become severely compressed.
Cauda equina syndrome requires emergency hospital admission and emergency surgery, because the longer it goes untreated, the greater the chance it will lead to permanent paralysis and incontinence.
Concussion
Concussion is a temporary injury to the brain caused by a bump, blow or jolt to the head. Very common in sports like martial arts, football, rugby. It can be mild or severe.Signs of a concussion usually appear within a few minutes or hours of a head injury. But occasionally they may not be obvious for a few days, so it’s important to look out for any problems in the days following a head injury.Symptoms include:
a headache that doesn’t go away or isn’t relieved with painkillers
dizziness
feeling sick or vomiting
memory loss – you may not remember what happened before or after the injury
clumsiness or trouble with balance
unusual behaviour – you may become irritated easily or have sudden mood swings
feeling stunned, dazed or confused
changes in your vision – such as blurred vision, double vision or “seeing stars”
being knocked out or struggling to stay awake
Concussion can be harder to spot in babies and young children.
One of the main things to look for is a change in their normal behaviour after a head injury, such as crying a lot, a change in their feeding or sleeping habits, or a loss of interest in people or objects.
When to go to hospital
Go to your nearest accident and emergency (A&E) department if you’ve injured your head and have:
woken up after being knocked out
problems with your memory
a headache that doesn’t go away
been vomiting since the injury
changes in your behaviour, such as becoming more irritable
had an operation on your brain in the past or are taking blood-thinning medicine such as warfarin
been drinking alcohol or taking recreational drugs
In these cases, you should be checked by a health professional trained in assessing head injuries. They’ll decide if you need a brain scan to rule out a serious brain injury.
When to an ambulance
Call for an ambulance if someone has injured their head and has:
been knocked out and hasn’t woken up
difficulty staying awake
problems with understanding, speaking, writing, walking or balance
numbness or weakness in part of their body
problems with their vision
clear fluid coming from their ears or nose
bleeding from their ears or bruising behind one or both ears
a black eye with no obvious damage around the eyes
a fit (seizure)
hit their head in a serious accident, such as a car crash
Also call for an ambulance if someone needs to go to hospital but you can’t get them there safely.
Cancer
It’s important to be aware of any unexplained changes to your body, such as the sudden appearance of a lump, blood in your urine, or a change to your usual bowel habits.
These symptoms are often caused by other, non-cancerous illnesses, but it’s important to seek medical support so they can investigate.
Bleeding
You should also see your GP if you have any unexplained bleeding, such as:
blood in your urine
bleeding between periods
bleeding from your bottom
blood when you cough
blood in your vomit
MolesSee your doctor if you have a mole that:
changes shape or looks uneven
changes colour, gets darker or has more than 2 colours
starts itching, crusting, flaking or bleeding
gets larger or more raised from the skin
Any of the above changes means there’s a chance you have malignant melanoma, a form of skin cancer.
Unexplained weight loss
You should also see your doctor if you’ve lost a lot of weight over the last couple of months that cannot be explained by changes to your diet, exercise or stress.
These symptoms can be related to cancer.
If you are not sure and have got any questions, please see your doctor for further examination.
Osteoarthritis is the most common cause of pain and disability in knees. In the knee joint, smooth articulate cartilage, called surface cartilage, covers the ends of the femur (thigh bone) and tibia (shin bone). Between the two bones sits a second type of cartilage, called menisci, which acts as a shock absorber. Joint fluid also lubricates the knee joint. Knee osteoarthritis (OA) is often characterized by knee pain and functional limitation and is widely understood to imply that symptoms are due to progressive structural damage. While age is a major risk factor for osteoarthritis of the knee, young people can get it, too. For some individuals, it may be hereditary. For others, osteoarthritis of the knee can result from previous injury or infection or even from being overweight. A full assessment is essential and can help to determine the right treatment plan, which may include these non-invasive options. X-rays, MRI and knee arthroscopy are just complement exams that can also be considered.
Knee osteoarthritis can be painful and debilitating, and the pain is often blamed on structural damage, with people frequently given scans and told that their knees are ‘bone on bone,’ leading them to believe that a knee replacement is inevitable.
However, new studies like the paper authored by Curtin University and published in British Journal of Sports Medicine has shed light on people living with knee osteoarthritis who may be needlessly suffering or receiving the wrong treatments for their symptoms, recommending a major change in how osteoarthritis is understood and treated. The paper suggests three steps that are needed to change the way healthcare professionals understand and manage knee osteoarthritis
The study pointed out that most people with osteoarthritis around the globe are not receiving the best practice care, including education, strengthening exercises, physical activity and weight management, that they require. Greater support from the health system is needed. The paper expressed that people with osteoarthritis are often provided potentially risky treatments with limited benefit such as opioid medication, injections, and arthroscopic surgery to manage their pain.
Researchers suggest that people with osteoarthritis need health professionals to coach them to develop a positive mindset, engage with exercise, and learn how to manage possible flare-ups. To facilitate a shift in the treatment of osteoarthritis, important changes need to occur at the health system level such as funding, and better reimbursement for exercise, weight loss and education programs for osteoarthritis care. They also report it is critical to spread the message to international and national healthcare professionals and the general public to change society’s misconceptions about knee osteoarthritis.
The key message is how exercises and life style changes can help to reduce/ manage knee pain caused by osteoarthritis.
Marco Ruas in action using a heel hook. Japan, 1998.
A heel hook is a leg lock affecting multiple joints, and is applied by transversely twisting the foot either medially or laterally. The torsional force puts severe torque on the ankle, which in turn transfers torque to the knee where the ACL has got an important function.
Heel hooks and other leg logs are featured, with various levels of restrictions, in combat sports and martial arts related with grappling such as Sambo, Brazilian Jiu-Jitsu, catch wrestling, Brazilian luta livre, mixed martial arts (MMA), Shootwrestling and submission wrestling, but are banned in some sports featuring joint locks such as judo.
The heel hook is a leg lock but the mechanism of action is completely different from an Achilles lock / straight lock. Heel hooks require rotational forces targeting different ligaments and transfer the forces to knee quickly and its effects can cause severe damage due to the extreme articular forces applied in a short period of time.
Here you can see the 3 factors that show why the heel hook is an effective/ dangerous submission and its mechanics is completely different from a traditional straight ankle lock.
1- There is no antagonist muscle to protect the joint. Antagonistic muscle – is a muscle that opposes the action of another. When you are applying an armbar the biceps and pectorals major (chest muscle) opposes the action of the amber applied, therefore, your opponent can resist to the armbar. There is no such thing with heel hooks due to its complex mechanics that applies a dynamic torsional force into the joint.
2- Reduced range of motion. If you are suffering an armbar you can resist due to the factor number 1 (antagonist muscle) and the angle of the joint (elbow) that has a good range of motion (see below). There is no such thing with heel hooks due to multiple lock systems used that restrict the range of motion considerably.
3- Articular forces transferred quickly. Well, we have got a submission with no antagonist muscle to resist and reduced range of motion. If an articular force is applied it will be transferred quickly into the joint, reducing the time for a good defense. It is not a surprise how fighters get injured when training/ competing using heel hooks.
Good fighters defend heel hooks through proactive measures: avoiding unnecessary exposure of the heel/ legs and using good timing so angles can be adjusted quickly, movements can be changed and a fatal attack can be prevented.
One of the great pioneers of modern MMA, Brazilian fighter Marco Ruas, UFC 7 winner after 3 fights and the founder of Ruas Vale Tudo, a hybrid form combining various disciplines of striking and grappling used heel hooks to obtain some of his victories. Ruas was the first complete MMA fighter which eventually evolved into today’s mixed martial arts competition.
John Danaher, (we will write an article about him), black belt in Brazilian jiu jitsu and one of the first students of Renzo Gracie when Renzo moved to US from Brazil, in the last few years, has developed an effective and logical system that can be seen when his students compete on the mats. It shows as a proper use of biomechanics can improve performance in competitions.
Football is the most popular sport in the world. But with sport, often comes injury. And unlike the pros, if you injure yourself during a match at your local park, there’s no medical team waiting for you .
Today we will discuss some of the most common injuries you might pick up on the pitch and what you can do to avoid theses injuries. It’s no surprise that the most common football injuries tend to affect your lower body due to tackling, running, shooting, twisting and turning, jumping or landing. You might also get an injury from using the same muscles repeatedly (overuse),
Ligament sprains (mainly ankle sprains)
Ligament sprains are the most common injury reported, accounting for more than 30 percent of all injuries, with the lateral ligaments of the ankle and medial collateral ligaments of the knee most commonly affected.
Concussions
Football is a sport that requires direct contact. With contact and competitive tackles we have trauma. Concussions make up 7.4 percent of all injuries in college football players.
Hamstrings strain
Your hamstrings are the three large and powerful muscles at the back of your thigh. They produce a driving force during acceleration when you run. Playing football often involves quick changes of pace, going from a complete stop to quick speed in just a couple of seconds. If your hamstrings don’t have enough length (from stretching) or strength, they can become quickly overloaded which could cause an injury.
To help prevent a hamstring strain, make sure to stretch them and use a foam roller regularly. A foam roller is a cylindrical device you use to massage and relieve sore and tight muscles. It can also help to work on strengthening your hamstring muscles using exercises such as deadlifts, leg curls and hamstring bridges, alongside some sport-specific speed drills.
Groin strain
When you’re on the pitch, kicking, twisting running or jumping could injure your inner thigh muscles (also known as your adductors), resulting in a groin strain. To help prevent getting a groin strain from football, be sure to stretch your inner thighs regularly and include strengthening exercises such as adductor side bridges and side lunges in your exercise routine.
ACL injury
When you’re on the pitch, kicking, twisting running or jumping could injure your inner thigh muscles (also known as your adductors), resulting in a groin strain. To help prevent getting a groin strain from football, be sure to stretch your inner thighs regularly and include strengthening exercises such as adductor side bridges and side lunges in your exercise routine.
Torn meniscus
When you play football, you’re often running on an uneven surface and have to change direction at a moment’s notice. This means that the ligaments which stabilise your ankle joint could become overstretched, and could cause your ankle to roll inwards or outwards.










/cdn.vox-cdn.com/uploads/chorus_image/image/49151597/GettyImages-74197143.0.jpg)








/track-runners-609202313-5a2db0bec7822d003778d0fc.jpg)




