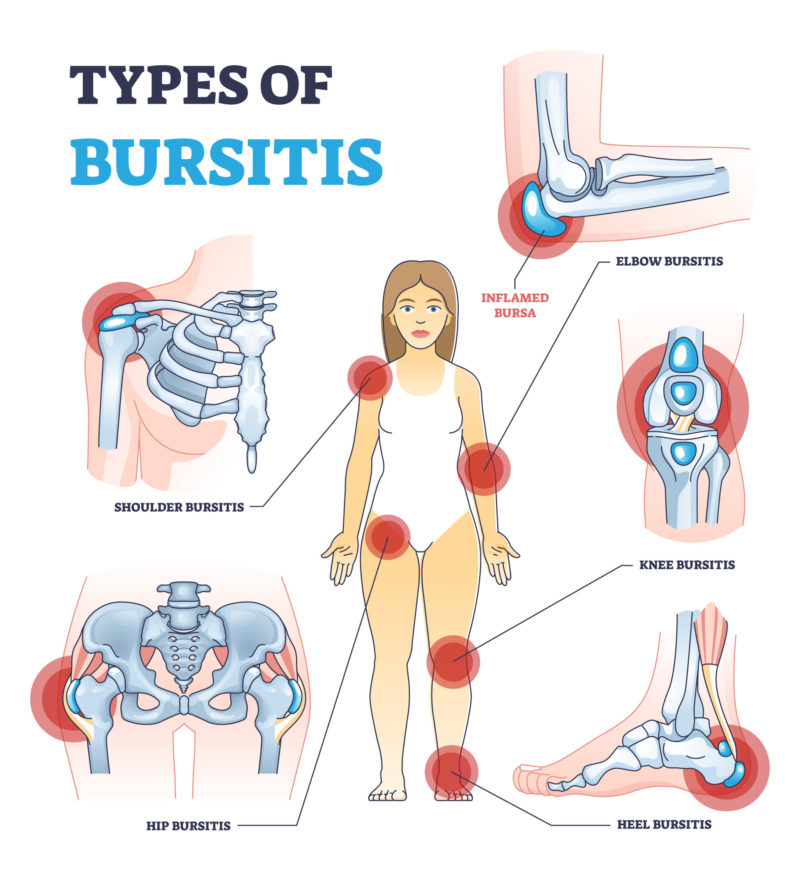
Bursitis is inflammation of a bursa, a closed, fluid-filled sac that works as a cushion and gliding surface to reduce friction between tissues of the body (normally bone corners in close contact with the skin and other soft tissues). The most common causes of bursitis are injury (direct trauma), overuse, biomechanical unbalances that lead to overuse, but it can also be caused by infection.
There are many bursas in the human body, from the feet joints to the shoulders, hips and hands. Pain, swelling, and tenderness near a joint are the most common signs of bursitis. Bursitis can be treated with rest and medicines to help with the inflammation. Antibiotics are used if infection is found.
To help bring down swelling and pain you can:
rest – try not to move the joint too much and avoid activities that put pressure on it
use ice – gently hold an ice pack (or a bag of frozen peas) wrapped in a tea towel on the area for around 10 minutes at a time and repeat every few hours during the day
take painkillers, to ease any pain
Physiotherapy- helps to improve unbalances
It may also help to put extra cushions around the affected joint while you sleep, to help protect and support it. See your doctor if you have a high temperature, or you feel hot and shivery
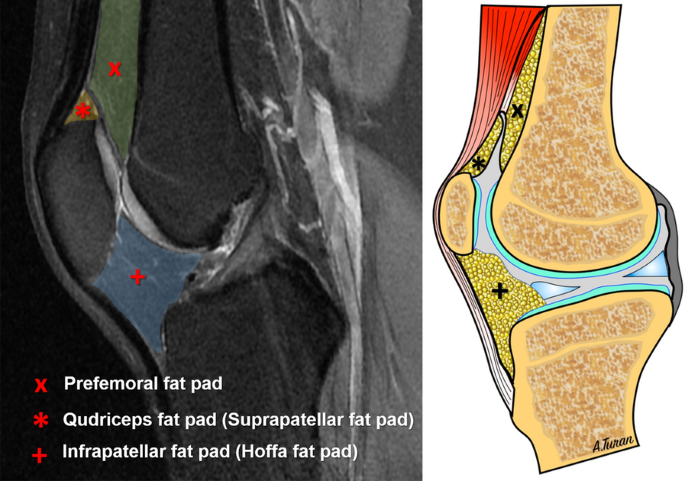
Hoffa’s syndrome, also known as infrapatellar fat pad syndrome, is a knee dysfunction which affects one of three pads of fatty soft tissue that lies under the kneecap (patella) and leads to pain at the front of the knee. The Hoffa’s fat pad acts as a protective cushion, which separates the kneecap from the shin and thigh bones.
It can be caused by a sudden trauma, such as a direct hit to your knee. However, it develops gradually more often over time if you repeatedly over-extend your knee. This is when your knee is forced beyond its fully straightened normal position.
Infrapatellar fat pad syndrome can be very painful.
The main symptoms are:
You’ll usually feel the pain at the front of your knee, around the bottom of your kneecap;
This pain may be worse when your leg is completely straight, or if you stand for a long time or when you go up or down stairs;
The area around the bottom of your kneecap may also feel very tender to the touch;
Joint hypermobility is when you have very flexible joints and it might causes you pain (you may think of yourself as being double-jointed).
A physiotherapist will usually test the flexibility of your joints using specific scores.
If it is too painful, they may also refer you for a blood test or X-ray to help rule out a joint dislocated.
There’s no cure for joint hypermobility syndrome as it has linked with genetics. Joint hypermobility syndrome can run in families and it cannot be prevented.
The main treatment is improving muscle strength of specific muscles and motor control so your joints are better protected.
Usually, the joints are loose and stretchy because the tissues that are part of the ligaments, the collagen, that strengthens the ligaments is different from other people’s.
Some people with hypermobility spectrum disorders do not have symptoms.
Most experts agree that joint hypermobility syndrome is part of a spectrum of hypermobility disorders which includes Ehlers-Danlos syndrome. (EDS).
EDS is different from hypermobility.
There are several types of EDS that may share some symptoms.
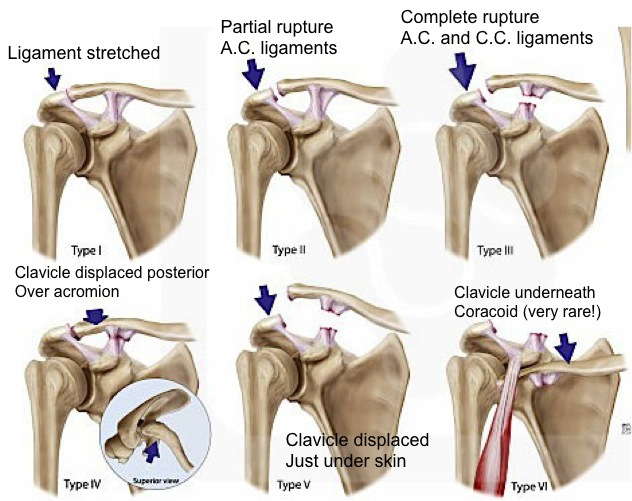
The Acromioclavicular Joint, or AC Joint, is one of four joints that comprises the Shoulder complex. The AC Joint is formed by the junction of the lateral clavicle and the acromion process of the scapula and is a gliding, or plane style synovial joint.
The origin of pain is normally a trauma (lateral fall, accidents,etc). Very common in rugby, judo, sambo and Brazilian Jiu Jitsu.
Symptoms of an AC joint injuryare
Shoulder or arm pain on the ACJ area.
A visible bump, bruise, or swelling on your shoulder.
Limited shoulder mobility when moving the arm upwards or crossing over the body.
Weakness in your shoulder or arm.
Pain when lying on the affected side.
A popping sound when you move your shoulder.
Levels of ACJ injury
Grades I-III are the most common (mild to moderated sprains). Grades IV-VI are very uncommon and are usually the result of a very high-energy injury such as one that might occur in a motor vehicle accident. Grades IV-VI are more severe.
Treatment:
First of all, the healing process must be respected. Time is needed.
Grades I-III are treated with physiotherapy. the most common (mild to moderated sprains). Grades IV-VI are very uncommon and are usually the result of a very high-energy injury such as one that might occur in a motor vehicle accident. Grades IV-VI are treated surgically because of the severe disruption of all the ligamentous support for the arm and shoulder.
Non-specific low back pain is usually categorized in 3 subtypes: acute, sub-acute and chronic low back pain. This subdivision is based on the duration of the back pain. Acute low back pain is an episode of low back pain for less than 6 weeks, sub-acute low back pain between 6 and 12 weeks and chronic low back pain for 12 weeks or more.
Low back pain (LBP) is the fifth most common reason for physician visits, which affects nearly 60-80% of people throughout their lifetime[6][7]. The lifetime prevalence of low back pain is reported to be as high as 84%, and the prevalence of chronic low back pain is about 23%, with 11-12% of the population being disabled by low back pain[1]. In the 2010 Global Burden of Disease study the global age-standardised point prevalence of LBP (from 0 to 100 years of age) was estimated to be 9.4%[8]. The same study showed that prevalence in 2010 was highest in western Europe followed by North Africa/Middle East, and lowest in the Caribbean followed by central Latin America.
Economically LBP is a huge burden, LBP causes more global disability than any other condition[8]. The cost of care for LBP has been reported (in the USA) to be over $50 billion annually[9]. Despite the intense focus and formal research on the care of non-specific LBP Pransky et al[10] reported a five fold increase in the prevalence of LBP over a 15 year period. It should be noted that most of the epidemiology/economic studies have been done in the western industrialised higher resourced countries and these figures will differ globally.
90% of people with LBP will recover in 3-4 months with no treatment.
70% of people with LBP will recover in 1 month with no treatment.
50% of people with LBP will recover in 2 weeks with no treatment.
5% of the remaining 10% will not respond to conservative care (such as physiotherapy)
The final 5% are the more challenging cases that don’t naturally improve that we as physiotherapists commonly see.
However these figures may be deceptive because although the pain may go away the the re-occurrence rate of LBP is extremely high and these individuals are likely to experience another episode of LBP within 3-6 months. Re-occurrence is a major problem with the re-occurrence rate being approximately 60%.
Non-specific low back pain accounts for over 90% of patients presenting to primary care[12] and these are the majority of the individuals with low back pain that present to physiotherapy.
Non-specific low back pain can caused by:
Traumatic injury
Lumbar sprain or strain
Postural strain
Cook et al (study ongoing 2015) studied risk factors for LBP pain:
First occurrence
Recurrent episode
Community setting
standing or walking >2hrs per dayfrequent moving or lifting >25 lbswidespread painlimpinghigher general health scores
other musculoskeletal complaintssitting, standing or walking >2hrs per dayfrequent moving or lifting >25 lbsstrength <50%depressionperceived inadequacy i.e. income, job
obesitypoor healthprior LBPpoor back endurancefrequent moving or lifting >25 lbsmanual jobsawkward posturemental distresspoor relationships at work
Leg pain is a frequent accompaniment to low back pain, arising from disorders of neural or musculoskeletal structures of the lumbar spine. Differentiating between different sources of radiating leg pain is important to make an appropriate diagnosis and identify the underlying pathology. Some specific causes of leg pain need to be managed in a different way to simple non-specific low back pain.
Low back pain is a symptom that accompanies several diseases. The diagnosis of non-specific low back pain implies no known pathoanatomical cause. Triage aims to exclude those cases in which the pain arises from either problems beyond the lumbar spine (eg, leaking aortic aneurysm); specific disorders affecting the lumbar spine (eg, epidural abscess, compression fracture, spondyloarthropathy, malignancy, cauda equina syndrome); or radicular pain, radiculopathy, or spinal canal stenosis. Remaining cases are non-specific low back pain. Several lumbar structures are plausible sources of pain (eg, the intervertebral disc, the facet joints), but clinical tests do not reliably attribute the pain to those structures.
Key message: The diagnosis of non-specific low back pain implies no known pathoanatomical cause.
Non-specific low back pain is defined as low back pain not attributable to a recognizable, known specific pathology. The place for surgery in chronic non-specific low back pain is very limited and its overuse has been criticized. Level of evidence 1A
For acute low back pain, most clinical practice guidelines agree on the use of reassurance, recommendations to stay active, brief education, paracetamol, non-steroidal anti-inflammatory drugs, spinal manipulation therapy, muscle relaxants (as second line drugs only, because of side-effects), and weak opioids (in selected cases). Level of evidence 1A
For chronic low back pain, the use of brief education about the problem, advice to stay active, non-steroidal anti-inflammatory drugs, weak opioids (short-term use), exercise therapy (of any sort), spinal manipulation are recommended and Self-management strategies. Level of evidence 1A
Myofascial pain is caused by a stimulus that sets off trigger points in your muscles. Triggers for myofascial pain can be factor that will affect the chemical balance of the body (stress and reduced sleep patterns). It will release some chemical substances in the body that can activate points of pain. This pattern is quite common with long term pain where normally the chemical balance is disturbed increasing the risk of long term pain.
Mechanical factors as long hours without movement in a static position can also increase muscle tightness and cause myofascial pain.
With myofascial pain, there are areas called trigger points. Normally, the patients report trigger points as “knots inside the muscle”. Trigger points are usually in the connective tissue (fascia) or in a tight muscle.
Myofascial pain syndrome is an ongoing or longer-lasting pain and can be managed with treatment.
Treatment includes aggravating factors management (stress management, improvement of sleep patterns); Gentle stretching and respiratory exercises; Soft tissue release; Massage; Acupuncture and dry needling; Aerobic exercise;
Physiotherapy is not only soft tissue release, manipulations and a couch.
In fact, a better understanding about pain (short term and long term) and the importance of exercises and training are playing a massive role in modern physiotherapy evidence based.
The importance of strength training is a popular subject nowadays. We wrote about the importance of strength training here.
However, another important form of training is often forgotten. We are talking about mobility training.
There is a reason why two of the most greatest fighters in the world, the Brazilian Jiu Jitsu master Rickson Gracie and the Swiss karateca Andy Hug (in memorian) trained mobility a lot.
Mobility is essential because it prepares our bodies and mind for the stress of demanding training. It is a vital contributor to reducing the risk of injuries as well as improving technique and range of movement. Mobility is also important because it allows you to function normally through your general daily activities.
Mobility training helps you develop a full range of motion in your arms, spine, trunk and legs. Exercises that enhance mobility also improve your joint health mainly with secondary positive effects in the muscles as well. Well-developed mobility gives you an advantage in martial arts, running, yoga and other physical activities as well as in day-to-day activities.
If you have stiff joints or is an advanced age athlete, mobility training can improve the range of motion of your joints and muscles. It can assist in improving posture in some cases. Mobility training can also alleviate daily aches and pains as well as improve our body awareness.
Mobility also plays a role in exercises that are purely strength driven like heavy squatting. Mobility is key for strength training and advancing to lifting more weight. Focus on improving your mobility and mobility-specific exercises to see improvements in your weightlifting or any other particular activity.
Exercises must be specific so it is important to note that strength training alone is not good enough to improve mobility.
Always remember: Your training must be specific, planned and structured to achieve your goals.
Mobility training should be take with caution when there is a history of joint instability, chronic dislocations and some medical conditions that affect joint health.
Today, #physio4fight will talk about squats. Find us on Facebook and leave your like so we can continue to do what we love: talk about exercises, fitness and physiotherapy.
A squat is a strength exercise in which the athlete lowers their hips from a standing position and then stands back up. Squat requires articular and muscular mobility, strength, balance and muscle control. During the descent of a squat, the hip and knee joints flex while the ankle joint dorsiflexes; conversely the hip and knee joints extend and the ankle joint plantarflexes when standing up. This is the basic form using the bodyweight but further resistance like dumbbells and kettlebells can also be added.
Some squat benefits you can see below:
1-It strengthens your core.
2-It reduces the risk of injury.
3-It rushes calories.
4-It strengthens the muscles of your lower body.
5-It boosts athletic ability and strength.
6-It variety helps with motivation.
7-It is a functional exercise.
Types of Squat.
There are a few but the most popular are:
Basic Squat
Single Leg Squat
Pistol Squat
Jump Squat
Bulgarian Squat
Overhead Squat
Landmine Squat
Spanish Squat
Squats are an excellent form of exercise using your own bodyweight and some level of mobility, flexibility and strength is required to complete this exercise . Furthermore, you must consider your fitness level, a gradual training progression and any particular limitation from a previous injury.
People are getting more active now (this is actually good) and sometimes we can get injured during or after exercising. Physiotherapy is normally advised and is an effective treatment.
However, there are scenarios that can be more complex and physiotherapy is not the answer. We are talking about red flags in physiotherapy.
Red flags are prognostic signs and symptoms suggestive of serious pathology. They are RARE (many physios work the whole life and do not see any or just a few cases) but can be concealed as a “joint/ muscle pain” but in fact they are something else and more sinister.
See some red flags below:
-Neck pain is quite common BUT if your symptoms are…
pain is getting much worse ( It can be individual and subjective due to multiple factors)
lack of co-ordination – for example trouble with tasks like buttoning a shirt
heaviness or weakness in your arms or legs
pins and needles (normally both arms but can affect just one arm) in an arm as well as pain
problems when walking
loss of bladder or bowel control
These can be signs of a more severe condition (cervical myelopathy) which can cause permanent damage to the spine if left untreated.
-Lower back pain is quite common BUT if you are having…
sciatica on both sides
weakness or numbness in both legs that is severe or getting worse
numbness around or under your genitals, or around your anus
finding it hard to start peeing, can’t pee or can’t control when you pee – and this isn’t normal for you
you don’t notice when you need to poo or can’t control when you poo – and this isn’t normal for you
Gait can also be affected
Theses symptoms are related to cauda equina. Cauda equina syndrome is a rare and severe type of spinal stenosis where all of the nerves in the lower back suddenly become severely compressed.
Cauda equina syndrome requires emergency hospital admission and emergency surgery, because the longer it goes untreated, the greater the chance it will lead to permanent paralysis and incontinence.
Concussion
Concussion is a temporary injury to the brain caused by a bump, blow or jolt to the head. Very common in sports like martial arts, football, rugby. It can be mild or severe.Signs of a concussion usually appear within a few minutes or hours of a head injury. But occasionally they may not be obvious for a few days, so it’s important to look out for any problems in the days following a head injury.Symptoms include:
a headache that doesn’t go away or isn’t relieved with painkillers
dizziness
feeling sick or vomiting
memory loss – you may not remember what happened before or after the injury
clumsiness or trouble with balance
unusual behaviour – you may become irritated easily or have sudden mood swings
feeling stunned, dazed or confused
changes in your vision – such as blurred vision, double vision or “seeing stars”
being knocked out or struggling to stay awake
Concussion can be harder to spot in babies and young children.
One of the main things to look for is a change in their normal behaviour after a head injury, such as crying a lot, a change in their feeding or sleeping habits, or a loss of interest in people or objects.
When to go to hospital
Go to your nearest accident and emergency (A&E) department if you’ve injured your head and have:
woken up after being knocked out
problems with your memory
a headache that doesn’t go away
been vomiting since the injury
changes in your behaviour, such as becoming more irritable
had an operation on your brain in the past or are taking blood-thinning medicine such as warfarin
been drinking alcohol or taking recreational drugs
In these cases, you should be checked by a health professional trained in assessing head injuries. They’ll decide if you need a brain scan to rule out a serious brain injury.
When to an ambulance
Call for an ambulance if someone has injured their head and has:
been knocked out and hasn’t woken up
difficulty staying awake
problems with understanding, speaking, writing, walking or balance
numbness or weakness in part of their body
problems with their vision
clear fluid coming from their ears or nose
bleeding from their ears or bruising behind one or both ears
a black eye with no obvious damage around the eyes
a fit (seizure)
hit their head in a serious accident, such as a car crash
Also call for an ambulance if someone needs to go to hospital but you can’t get them there safely.
Cancer
It’s important to be aware of any unexplained changes to your body, such as the sudden appearance of a lump, blood in your urine, or a change to your usual bowel habits.
These symptoms are often caused by other, non-cancerous illnesses, but it’s important to seek medical support so they can investigate.
Bleeding
You should also see your GP if you have any unexplained bleeding, such as:
blood in your urine
bleeding between periods
bleeding from your bottom
blood when you cough
blood in your vomit
MolesSee your doctor if you have a mole that:
changes shape or looks uneven
changes colour, gets darker or has more than 2 colours
starts itching, crusting, flaking or bleeding
gets larger or more raised from the skin
Any of the above changes means there’s a chance you have malignant melanoma, a form of skin cancer.
Unexplained weight loss
You should also see your doctor if you’ve lost a lot of weight over the last couple of months that cannot be explained by changes to your diet, exercise or stress.
These symptoms can be related to cancer.
If you are not sure and have got any questions, please see your doctor for further examination.
Osteoarthritis is the most common cause of pain and disability in knees. In the knee joint, smooth articulate cartilage, called surface cartilage, covers the ends of the femur (thigh bone) and tibia (shin bone). Between the two bones sits a second type of cartilage, called menisci, which acts as a shock absorber. Joint fluid also lubricates the knee joint. Knee osteoarthritis (OA) is often characterized by knee pain and functional limitation and is widely understood to imply that symptoms are due to progressive structural damage. While age is a major risk factor for osteoarthritis of the knee, young people can get it, too. For some individuals, it may be hereditary. For others, osteoarthritis of the knee can result from previous injury or infection or even from being overweight. A full assessment is essential and can help to determine the right treatment plan, which may include these non-invasive options. X-rays, MRI and knee arthroscopy are just complement exams that can also be considered.
Knee osteoarthritis can be painful and debilitating, and the pain is often blamed on structural damage, with people frequently given scans and told that their knees are ‘bone on bone,’ leading them to believe that a knee replacement is inevitable.
However, new studies like the paper authored by Curtin University and published in British Journal of Sports Medicine has shed light on people living with knee osteoarthritis who may be needlessly suffering or receiving the wrong treatments for their symptoms, recommending a major change in how osteoarthritis is understood and treated. The paper suggests three steps that are needed to change the way healthcare professionals understand and manage knee osteoarthritis
The study pointed out that most people with osteoarthritis around the globe are not receiving the best practice care, including education, strengthening exercises, physical activity and weight management, that they require. Greater support from the health system is needed. The paper expressed that people with osteoarthritis are often provided potentially risky treatments with limited benefit such as opioid medication, injections, and arthroscopic surgery to manage their pain.
Researchers suggest that people with osteoarthritis need health professionals to coach them to develop a positive mindset, engage with exercise, and learn how to manage possible flare-ups. To facilitate a shift in the treatment of osteoarthritis, important changes need to occur at the health system level such as funding, and better reimbursement for exercise, weight loss and education programs for osteoarthritis care. They also report it is critical to spread the message to international and national healthcare professionals and the general public to change society’s misconceptions about knee osteoarthritis.
The key message is how exercises and life style changes can help to reduce/ manage knee pain caused by osteoarthritis.













/track-runners-609202313-5a2db0bec7822d003778d0fc.jpg)
