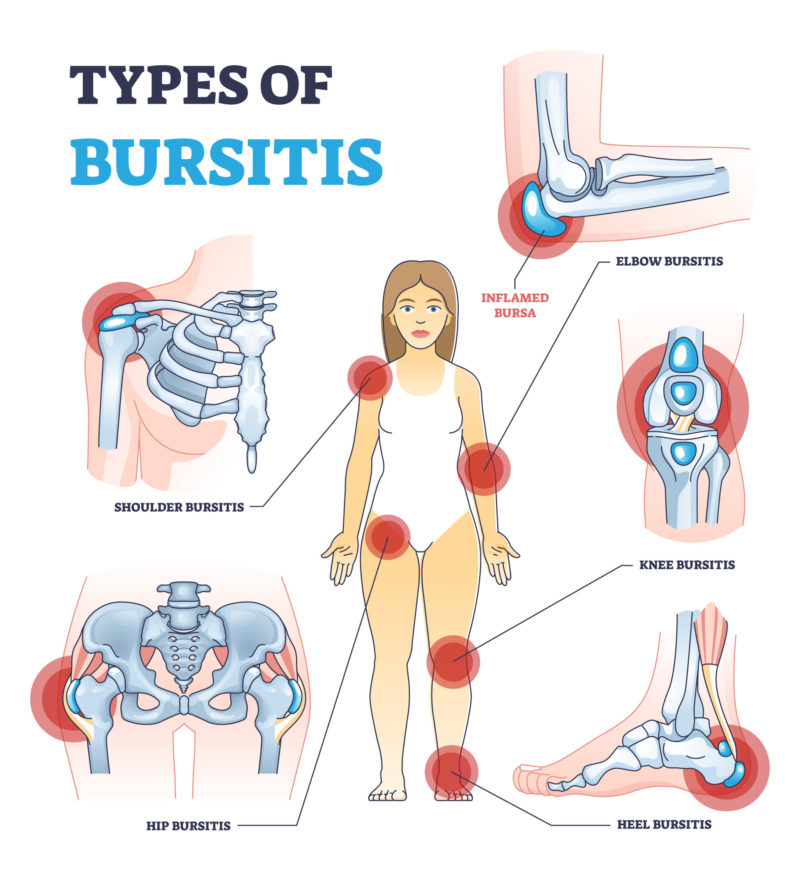
Bursitis is inflammation of a bursa, a closed, fluid-filled sac that works as a cushion and gliding surface to reduce friction between tissues of the body (normally bone corners in close contact with the skin and other soft tissues). The most common causes of bursitis are injury (direct trauma), overuse, biomechanical unbalances that lead to overuse, but it can also be caused by infection.
There are many bursas in the human body, from the feet joints to the shoulders, hips and hands. Pain, swelling, and tenderness near a joint are the most common signs of bursitis. Bursitis can be treated with rest and medicines to help with the inflammation. Antibiotics are used if infection is found.
To help bring down swelling and pain you can:
rest – try not to move the joint too much and avoid activities that put pressure on it
use ice – gently hold an ice pack (or a bag of frozen peas) wrapped in a tea towel on the area for around 10 minutes at a time and repeat every few hours during the day
take painkillers, to ease any pain
Physiotherapy- helps to improve unbalances
It may also help to put extra cushions around the affected joint while you sleep, to help protect and support it. See your doctor if you have a high temperature, or you feel hot and shivery
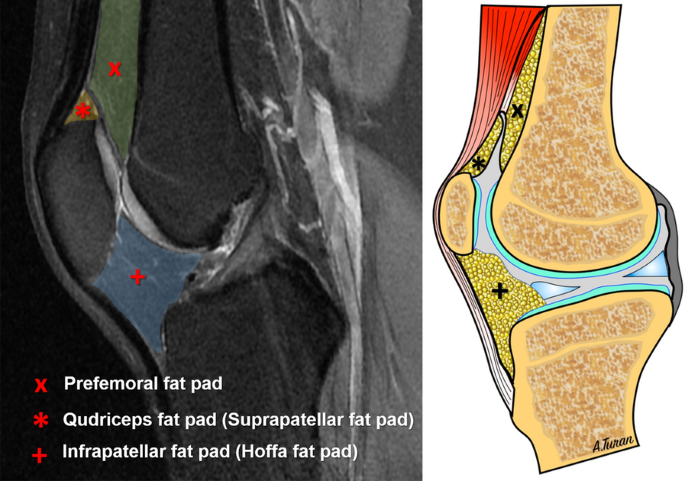
Hoffa’s syndrome, also known as infrapatellar fat pad syndrome, is a knee dysfunction which affects one of three pads of fatty soft tissue that lies under the kneecap (patella) and leads to pain at the front of the knee. The Hoffa’s fat pad acts as a protective cushion, which separates the kneecap from the shin and thigh bones.
It can be caused by a sudden trauma, such as a direct hit to your knee. However, it develops gradually more often over time if you repeatedly over-extend your knee. This is when your knee is forced beyond its fully straightened normal position.
Infrapatellar fat pad syndrome can be very painful.
The main symptoms are:
You’ll usually feel the pain at the front of your knee, around the bottom of your kneecap;
This pain may be worse when your leg is completely straight, or if you stand for a long time or when you go up or down stairs;
The area around the bottom of your kneecap may also feel very tender to the touch;
Joint hypermobility is when you have very flexible joints and it might causes you pain (you may think of yourself as being double-jointed).
A physiotherapist will usually test the flexibility of your joints using specific scores.
If it is too painful, they may also refer you for a blood test or X-ray to help rule out a joint dislocated.
There’s no cure for joint hypermobility syndrome as it has linked with genetics. Joint hypermobility syndrome can run in families and it cannot be prevented.
The main treatment is improving muscle strength of specific muscles and motor control so your joints are better protected.
Usually, the joints are loose and stretchy because the tissues that are part of the ligaments, the collagen, that strengthens the ligaments is different from other people’s.
Some people with hypermobility spectrum disorders do not have symptoms.
Most experts agree that joint hypermobility syndrome is part of a spectrum of hypermobility disorders which includes Ehlers-Danlos syndrome. (EDS).
EDS is different from hypermobility.
There are several types of EDS that may share some symptoms.
The Acromioclavicular Joint, or AC Joint, is one of four joints that comprises the Shoulder complex. The AC Joint is formed by the junction of the lateral clavicle and the acromion process of the scapula and is a gliding, or plane style synovial joint.
The origin of pain is normally a trauma (lateral fall, accidents,etc). Very common in rugby, judo, sambo and Brazilian Jiu Jitsu.
Symptoms of an AC joint injuryare
Shoulder or arm pain on the ACJ area.
A visible bump, bruise, or swelling on your shoulder.
Limited shoulder mobility when moving the arm upwards or crossing over the body.
Weakness in your shoulder or arm.
Pain when lying on the affected side.
A popping sound when you move your shoulder.
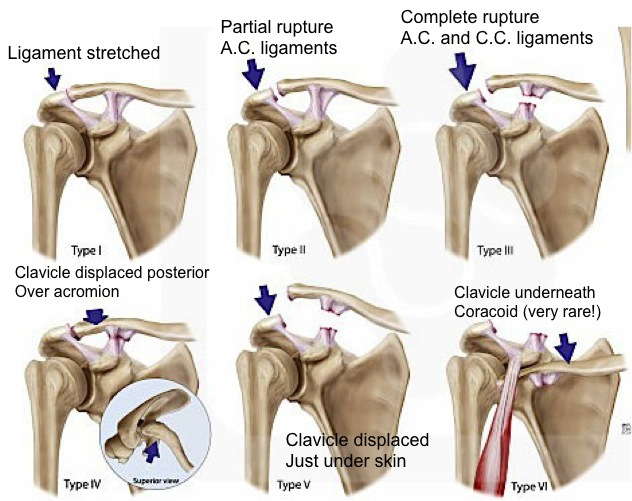
Levels of ACJ injury
Grades I-III are the most common (mild to moderated sprains). Grades IV-VI are very uncommon and are usually the result of a very high-energy injury such as one that might occur in a motor vehicle accident. Grades IV-VI are more severe.
Treatment:
First of all, the healing process must be respected. Time is needed.
Grades I-III are treated with physiotherapy. the most common (mild to moderated sprains). Grades IV-VI are very uncommon and are usually the result of a very high-energy injury such as one that might occur in a motor vehicle accident. Grades IV-VI are treated surgically because of the severe disruption of all the ligamentous support for the arm and shoulder.
Non-specific low back pain is usually categorized in 3 subtypes: acute, sub-acute and chronic low back pain. This subdivision is based on the duration of the back pain. Acute low back pain is an episode of low back pain for less than 6 weeks, sub-acute low back pain between 6 and 12 weeks and chronic low back pain for 12 weeks or more.
Low back pain (LBP) is the fifth most common reason for physician visits, which affects nearly 60-80% of people throughout their lifetime[6][7]. The lifetime prevalence of low back pain is reported to be as high as 84%, and the prevalence of chronic low back pain is about 23%, with 11-12% of the population being disabled by low back pain[1]. In the 2010 Global Burden of Disease study the global age-standardised point prevalence of LBP (from 0 to 100 years of age) was estimated to be 9.4%[8]. The same study showed that prevalence in 2010 was highest in western Europe followed by North Africa/Middle East, and lowest in the Caribbean followed by central Latin America.
Economically LBP is a huge burden, LBP causes more global disability than any other condition[8]. The cost of care for LBP has been reported (in the USA) to be over $50 billion annually[9]. Despite the intense focus and formal research on the care of non-specific LBP Pransky et al[10] reported a five fold increase in the prevalence of LBP over a 15 year period. It should be noted that most of the epidemiology/economic studies have been done in the western industrialised higher resourced countries and these figures will differ globally.
90% of people with LBP will recover in 3-4 months with no treatment.
70% of people with LBP will recover in 1 month with no treatment.
50% of people with LBP will recover in 2 weeks with no treatment.
5% of the remaining 10% will not respond to conservative care (such as physiotherapy)
The final 5% are the more challenging cases that don’t naturally improve that we as physiotherapists commonly see.
However these figures may be deceptive because although the pain may go away the the re-occurrence rate of LBP is extremely high and these individuals are likely to experience another episode of LBP within 3-6 months. Re-occurrence is a major problem with the re-occurrence rate being approximately 60%.
Non-specific low back pain accounts for over 90% of patients presenting to primary care[12] and these are the majority of the individuals with low back pain that present to physiotherapy.
Non-specific low back pain can caused by:
Traumatic injury
Lumbar sprain or strain
Postural strain
Cook et al (study ongoing 2015) studied risk factors for LBP pain:
First occurrence
Recurrent episode
Community setting
standing or walking >2hrs per dayfrequent moving or lifting >25 lbswidespread painlimpinghigher general health scores
other musculoskeletal complaintssitting, standing or walking >2hrs per dayfrequent moving or lifting >25 lbsstrength <50%depressionperceived inadequacy i.e. income, job
obesitypoor healthprior LBPpoor back endurancefrequent moving or lifting >25 lbsmanual jobsawkward posturemental distresspoor relationships at work
Leg pain is a frequent accompaniment to low back pain, arising from disorders of neural or musculoskeletal structures of the lumbar spine. Differentiating between different sources of radiating leg pain is important to make an appropriate diagnosis and identify the underlying pathology. Some specific causes of leg pain need to be managed in a different way to simple non-specific low back pain.
Low back pain is a symptom that accompanies several diseases. The diagnosis of non-specific low back pain implies no known pathoanatomical cause. Triage aims to exclude those cases in which the pain arises from either problems beyond the lumbar spine (eg, leaking aortic aneurysm); specific disorders affecting the lumbar spine (eg, epidural abscess, compression fracture, spondyloarthropathy, malignancy, cauda equina syndrome); or radicular pain, radiculopathy, or spinal canal stenosis. Remaining cases are non-specific low back pain. Several lumbar structures are plausible sources of pain (eg, the intervertebral disc, the facet joints), but clinical tests do not reliably attribute the pain to those structures.
Key message: The diagnosis of non-specific low back pain implies no known pathoanatomical cause.
Non-specific low back pain is defined as low back pain not attributable to a recognizable, known specific pathology. The place for surgery in chronic non-specific low back pain is very limited and its overuse has been criticized. Level of evidence 1A
For acute low back pain, most clinical practice guidelines agree on the use of reassurance, recommendations to stay active, brief education, paracetamol, non-steroidal anti-inflammatory drugs, spinal manipulation therapy, muscle relaxants (as second line drugs only, because of side-effects), and weak opioids (in selected cases). Level of evidence 1A
For chronic low back pain, the use of brief education about the problem, advice to stay active, non-steroidal anti-inflammatory drugs, weak opioids (short-term use), exercise therapy (of any sort), spinal manipulation are recommended and Self-management strategies. Level of evidence 1A
Myofascial pain is caused by a stimulus that sets off trigger points in your muscles. Triggers for myofascial pain can be factor that will affect the chemical balance of the body (stress and reduced sleep patterns). It will release some chemical substances in the body that can activate points of pain. This pattern is quite common with long term pain where normally the chemical balance is disturbed increasing the risk of long term pain.
Mechanical factors as long hours without movement in a static position can also increase muscle tightness and cause myofascial pain.
With myofascial pain, there are areas called trigger points. Normally, the patients report trigger points as “knots inside the muscle”. Trigger points are usually in the connective tissue (fascia) or in a tight muscle.
Myofascial pain syndrome is an ongoing or longer-lasting pain and can be managed with treatment.
Treatment includes aggravating factors management (stress management, improvement of sleep patterns); Gentle stretching and respiratory exercises; Soft tissue release; Massage; Acupuncture and dry needling; Aerobic exercise;
Running is probably one of the oldest forms of physical activities.
Tip 1: A physical activity is different from a exercise. Furthermore, there are general exercises and specific exercises.
The study of different running styles and classifications is a very popular subject now but some people still do not understand what they are. After all, running is just running?
Well, things are a little bit more complex. More research is needed to determine if different foot strikes give runners any advantage during their races.
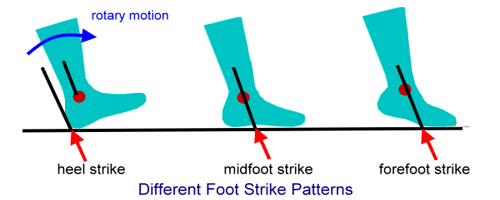
Basically, there are important mechanical differences between midfoot strike, forefoot strike, and heel strike (the 3 main styles of running). See image above.
Forefoot striker
Forefoot runners land on the forefoot ( ball of their foot or on their toes). As they stride, their heel may not hit the ground at all. This stride can cause your body to lean forward. It may put additional strain on your toes and calf muscles.
Landing on your forefoot ( the balls of the feet and toes) is considered effective. But landing on the toes may cause injury if you’re a distance runner. Although it’s effective for sprinting and short bursts of speed, landing too far forward on your toes isn’t recommended for longer distances. It could lead to shin splints or other injuries.
Common injuries? You may be more prone to injure your ankle, Achilles tendon or to have plantar fasciitis
Midfoot strike
Considered the most “neutral” strike, midfoot strikers land in the center of their foot, with their body weight evenly distributed to the ankles, hips, back, and knees. Midfoot runners may be able to run efficiently and with speed.
Common injuries? You may experience foot, ankle, or Achilles pain at some point.
Heel striker
As mentioned, heel strikers hit the ground with their heels first before the rest of their foot hits the ground. This can put additional strain on the knees.
Common injuries? You may be more prone to knee and hip pain.
Tip 2: Any changes to your running form or trainers should be done gradually. The running style should fit your body type and your anatomy.
Tip 3: A sudden increase in training mileage or a quick uptick in speed training means you overwork the muscles when they’re not quite ready, which can lead to unnecessary pain.
Physiotherapy is not only soft tissue release, manipulations and a couch.
In fact, a better understanding about pain (short term and long term) and the importance of exercises and training are playing a massive role in modern physiotherapy evidence based.
The importance of strength training is a popular subject nowadays. We wrote about the importance of strength training here.
However, another important form of training is often forgotten. We are talking about mobility training.
There is a reason why two of the most greatest fighters in the world, the Brazilian Jiu Jitsu master Rickson Gracie and the Swiss karateca Andy Hug (in memorian) trained mobility a lot.
Mobility is essential because it prepares our bodies and mind for the stress of demanding training. It is a vital contributor to reducing the risk of injuries as well as improving technique and range of movement. Mobility is also important because it allows you to function normally through your general daily activities.
Mobility training helps you develop a full range of motion in your arms, spine, trunk and legs. Exercises that enhance mobility also improve your joint health mainly with secondary positive effects in the muscles as well. Well-developed mobility gives you an advantage in martial arts, running, yoga and other physical activities as well as in day-to-day activities.
If you have stiff joints or is an advanced age athlete, mobility training can improve the range of motion of your joints and muscles. It can assist in improving posture in some cases. Mobility training can also alleviate daily aches and pains as well as improve our body awareness.
Mobility also plays a role in exercises that are purely strength driven like heavy squatting. Mobility is key for strength training and advancing to lifting more weight. Focus on improving your mobility and mobility-specific exercises to see improvements in your weightlifting or any other particular activity.
Exercises must be specific so it is important to note that strength training alone is not good enough to improve mobility.
Always remember: Your training must be specific, planned and structured to achieve your goals.
Mobility training should be take with caution when there is a history of joint instability, chronic dislocations and some medical conditions that affect joint health.
Hip pain has many causes that could be related from specific conditions (bursitis, tendinopathies, osteoarthritis,etc) to reduced mobility , direct trauma, overuse and reduced motor control. As we know these days, pain is now always caused by trauma or imaging findings.
One of these conditions is called FAI.Femoroacetabular impingement (FAI) (also called hip impingement) is a motion-related clinical disorder of the hip involving premature contact between the acetabulum and the proximal femur and which results in particular symptoms, clinical signs and imaging findings.
As with many conditions and based on a modern physiotherapy approach, we should correlate lifestyle, symptoms and its effects with pain levels and clinical findings. Imaging findings alone are not the reason for musculoskeletalpain.
It is not known how many people have FAI. Often, many people may live long, active lives with FAI and never have problems. Degenerative changes and osteoarthritis may/ may not develop in the long-term as a result of this abnormal contact. Once again, many people may live long and actives lives with osteoarthritis and never have problems.
In FAI, bone overgrowth — called bone spurs — develop around the femoral head and/or along the acetabulum. This extra bone causes abnormal contact between the hip bones, and prevents them from moving smoothly during activity. Over time, this can result affect the labrum and the articular cartilage.
What does a hip impingement feel like? Hip or groin pain related to certain movements or positions (sitting during long hours, sitting on a low chair, playing guard (BJJ, picture above)), stiffness in the groin, pain in the front of the thigh or down the buttocks, popping or clicking in the front of the hip as you move, and some loss of your hip’s mobility.
Differential diagnosis and red flags: Acute hip pain due to tumour, infection, septic arthritis, osteomyelitis, fracture and avascular necrosis are red flag conditions(see what red flags are here) that should be ruled out. In athletes, other causes of hip pain include inguinal pathology, adductor pathology and athletic pubalgia.
Treatment of hip impingement/femoroacetabular impingement begins with conservative, non-surgical methods. Rest, activity modifications, careful use of anti-inflammatory medications, and a physiotherapy are often successful in alleviating symptoms. Some authors suggest that improving neuromuscular function of the hip should be a goal of conservative protocols for FAI syndrome due to weakness of deep hip musculature and an expected subsequent reduction in dynamic stability of the hip joint. A good physiotherapist definitely can help you.
Surgery is normally the last resource and arthroscopy is the most common surgical procedure for FAI discussed in the literature.
Today, #physio4fight will talk about basic strength training exercises. Find us on Facebook and leave your like so we can continue to do what we love: talk about the importance of exercises, fitness and physiotherapy.
Strength training has got many benefits: maintain muscle tissue, increase strength, improve bone health, control body fat, decrease risk of injury are some of them . It can also help you manage or lose weight, and it can increase your metabolism to help you burn more calories. Strength training may enhance your quality of life and improve your ability to do everyday activities.
This is particular important when we are aging and losing muscle mass and tone. Strength training can help us how to manage that. Do not forget that muscle strength can be worked in multiple ways and using multiples tools and equipment or only your body weight.
Normally, some level of mobility is also necessary so do not forget to improve your mobility as well.
Gradually increase the intensity and loading of your workouts as your fitness improves and let your body rest from time to time to help prevent injuries.
Note 1: This is just a guide and DOES NOT replace a session with a physiotherapist. Find a good physiotherapist in your area to help you.
Note 2: If you have not exercised for a while, Delayed onset muscle soreness is expected. Learn more about it here.
Basic exercises below:
Bridge
Plank
Push ups
Pull down using elastic band(you can do this exercise kneeling for better latissimus dorsi activation). A good progression after this exercise (if you are interested) could be assisted pull ups.